- (731) 423-8200
- 1877-284-3135

- Contact Us
The Preoperative Cardiac Clearance Clinic
A data-driven look at how our specialized service enhances patient safety and streamlines surgical scheduling.




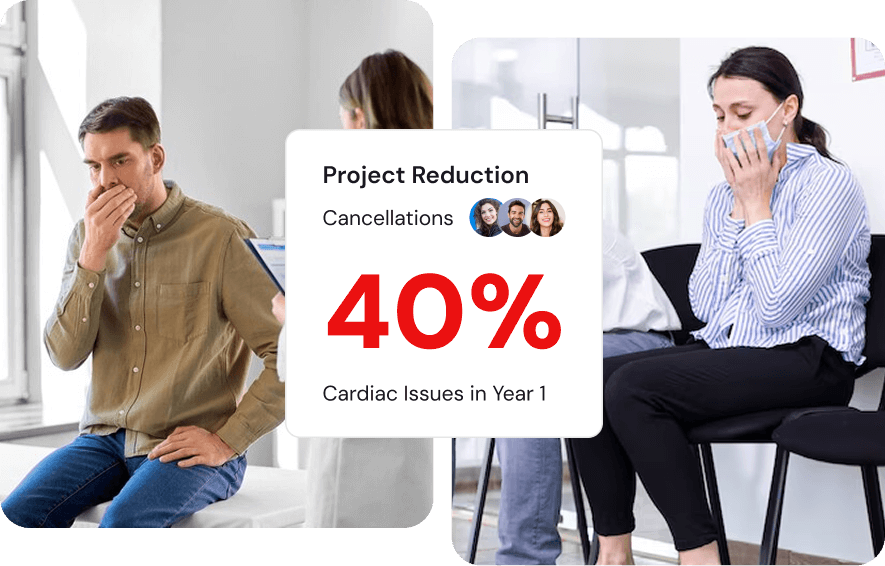
Cancellations
Projected Impact on Surgical Cancellations
By proactively managing cardiac risk, we anticipate a significant reduction in last-minute cancellations.
Projected Reduction in Cancellations Due to Cardiac Issues in Year 1
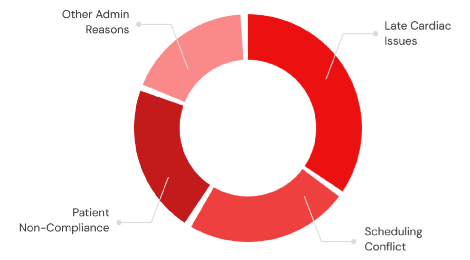
The Challenge:
Why Surgeries Are Delayed
A significant portion of preventable surgical delays stem from unresolved cardiac concerns discovered late in the preoperative process. Our clinic directly addresses this bottleneck.
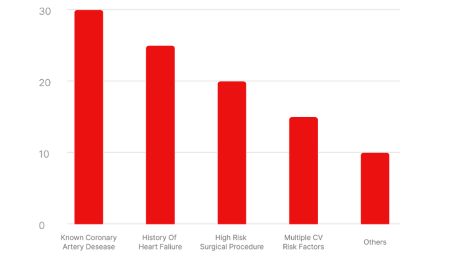
Target Patient
Population by Referral
The clinic serves a diverse group of patients, primarily those with known risk factors who require specialized assessment before their procedures.
Patient Journey
Our Solution: A Streamlined Patient Journey
01
Referral Received
From Surgical or Primary Care Clinic
02
Expedited Appointment
Scheduled within 3-5 business days
03
Specialized Evaluation
Risk stratification & testing plan
04
Optimization & Clearance
Clear communication back to surgeon
Core Benefits
Core Benefits of the Service Line

Dedicated Expertise
Access to board-certified cardiologists focused solely on perioperative care, ensuring the highest standard of evaluation and management.
Enhanced Efficiency
Streamlined scheduling and communication drastically reduce the time from referral to surgical clearance, minimizing costly delays.

Improved Safety
Proactive risk mitigation and patient optimization lead to a measurable reduction in perioperative cardiac events and better outcomes.
Terminologies
Key Medical Terminology
The line color style will help you to highlight the content in the accordion.
The line color style will help you to highlight the content in the accordion.
The line color style will help you to highlight the content in the accordion.
The line color style will help you to highlight the content in the accordion.
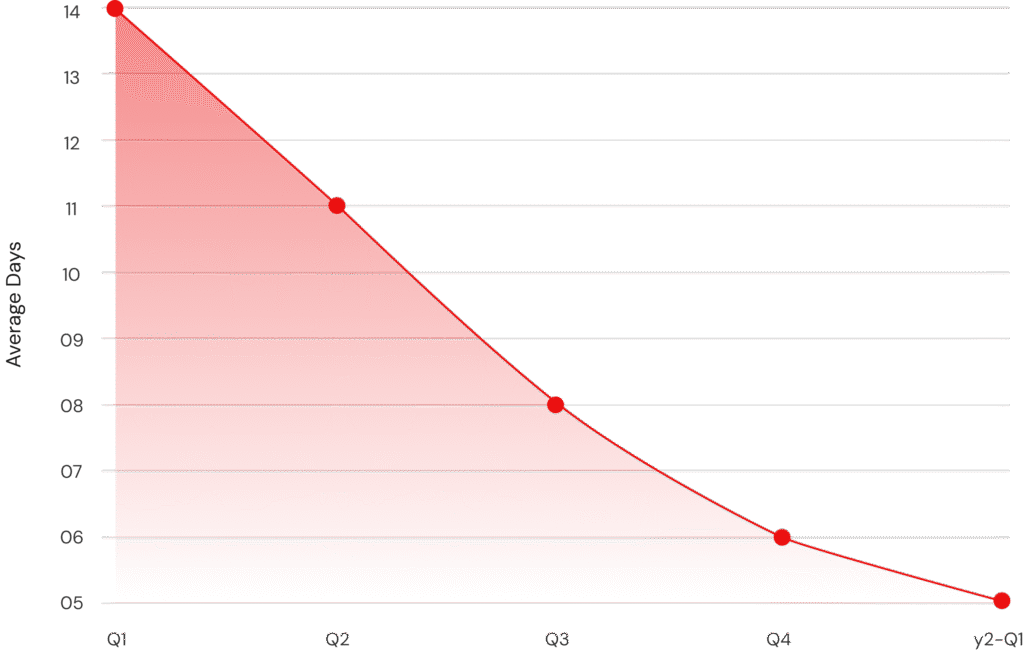
Efficiency
Projected Efficiency Gains
We project a steady decrease in the average time to clearance as our processes mature and referral patterns stabilize over the first year of operation.
Frequently Asked Questions
Answers You Can Trust
We’ve gathered the most common questions to help you make informed and confident decisions.
This is a procedure done on the heart. In it, a doctor inserts a thin plastic tube (catheter) (KATH'eh-ter) into an artery or vein in the arm or leg. From there it can be advanced into the chambers of the heart or into the coronary arteries.
Catheters are also used to inject dye into the coronary arteries. This is called coronary angiography (an"je-OG'rah-fe) or coronary arteriography (ar-te"re-OG'rah-fe). This is done to see if the arteries have blockage that could cause a heart attack. This test can measure blood pressure within the heart and how much oxygen is in the blood. It's also used to get information about the pumping ability of the heart muscle. Catheters with a balloon on the tip are used in the procedure called percutaneous transluminal coronary angioplasty (per"ku-TA'ne-us tranz-LU'min-al KOR'o-nair-e AN'je-o-plas-te) (PTCA). Catheterization is also done on infants and children to examine or treat congenital (kon-JEN'ih-tal) heart defects.
A stent is a wire mesh tube used to prop open an artery that's recently been cleared using angioplasty. The stent is collapsed to a small diameter and put over a balloon catheter. It's then moved into the area of the blockage. When the balloon is inflated, the stent expands, locks in place and forms a scaffold. This holds the artery open. The stent stays in the artery permanently, holds it open, improves blood flow to the heart muscle and relieves symptoms (usually chest pain).
In certain patients, stents reduce the renarrowing that occurs after balloon angioplasty or other procedures that use catheters. Stents also help restore normal blood flow and keep an artery open if it's been torn or injured by the balloon catheter.
Patients who've had a stent procedure must take one or more blood-thinning agents. Examples are aspirin and ticlopidine or clopidogrel. Aspirin is used indefinitely; one of the other 6 - 12 months. For the next four weeks a magnetic resonance imaging (MRI) scan should not be done without a cardiologist's approval. But metal detectors don't affect the stent.
Atherectomy (ath"er-EK'to-me) is a procedure to remove plaque from arteries. Plaque is the buildup of fat, cholesterol and other substances in an artery's inner lining.
Coronary atherectomy removes plaque from the arteries supplying blood to the heart muscle. It uses a laser catheter, or a rotating shaver ("burr" device on the end of a catheter). The catheter is inserted into the body and advanced through an artery to the area of narrowing. Other devices are dissectional catheterectomy, catheters that shave off the plaque, or laser catheters that vaporize the plaque. Balloon angioplasty or stenting may be used after an atherectomy.
Persons with plaque buildups in the carotid (kah-ROT'id) arteries or major arteries of the neck are at higher risk for stroke. Carotid endarterectomy (end"ar-ter-EK'to-me) is an effective surgical procedure that can help them. It removes the plaque to reduce the risk of stroke.
Coronary atherectomy removes plaque from the arteries supplying blood to the heart muscle. It uses a laser catheter, or a rotating shaver ("burr" device on the end of a catheter). The catheter is inserted into the body and advanced through an artery to the area of narrowing. Other devices are dissectional catheterectomy, catheters that shave off the plaque, or laser catheters that vaporize the plaque. Balloon angioplasty or stenting may be used after an atherectomy.
Persons with plaque buildups in the carotid (kah-ROT'id) arteries or major arteries of the neck are at higher risk for stroke. Carotid endarterectomy (end"ar-ter-EK'to-me) is an effective surgical procedure that can help them. It removes the plaque to reduce the risk of stroke.
A pacemaker is a small unit that is implanted under the skin and uses batteries to help your heart beat more regularly through the use of small electric stimulation that helps control your heartbeat.
Coronary angioplasty is a procedure that opens blocked arteries and allows blood to flow to your heart muscle. Angioplasty is not surgery. It opens a clogged coronary artery by inflating a tiny balloon in it. This information sheet discusses what the procedure is, who needs it, how it is done, and recovery afterwards.
A stent may be used instead of -- or along with -- angioplasty. Stents are used depending on certain features of the artery blockage. This includes the size of the artery and where the blockage is. Stenting is a fairly common procedure; in fact, it now represents 70-90 percent of procedures.
Yes. Reclosure (restenosis) is also a problem with the stent procedure. In recent years doctors have used new types of stents called drug-eluting stents. These are coated with drugs that are slowly released and help keep the blood vessel from reclosing. These new stents have shown some promise for improving the long-term success of this procedure.
To date there's no evidence of long-term complications from having a permanent stent.
A heart attack occurs when the blood supply to part of the heart muscle itself -- the myocardium -- is severely reduced or stopped. The medical term for heart attack is myocardial infarction. The reduction or stoppage happens when one or more of the coronary arteries supplying blood to the heart muscle is blocked. This is usually caused by the buildup of plaque (deposits of fat-like substances), a process called atherosclerosis. The plaque can eventually burst, tear or rupture, creating a "snag" where a blood clot forms and blocks the artery. This leads to a heart attack. A heart attack is also sometimes called a coronary thrombosis or coronary occlusion.
If the blood supply is cut off for more than a few minutes, muscle cells suffer permanent injury and die. This can kill or disable someone, depending on how much heart muscle is damaged.
Sometimes a coronary artery temporarily contracts or goes into spasm. When this happens the artery narrows and blood flow to part of the heart muscle decreases or stops. We're not sure what causes a spasm. A spasm can occur in normal-appearing blood vessels as well as in vessels partly blocked by atherosclerosis. A severe spasm can cause a heart attack.
If the blood supply is cut off for more than a few minutes, muscle cells suffer permanent injury and die. This can kill or disable someone, depending on how much heart muscle is damaged.
Sometimes a coronary artery temporarily contracts or goes into spasm. When this happens the artery narrows and blood flow to part of the heart muscle decreases or stops. We're not sure what causes a spasm. A spasm can occur in normal-appearing blood vessels as well as in vessels partly blocked by atherosclerosis. A severe spasm can cause a heart attack.
Congestive heart failure is usually caused by a previous heart attack which causes the heart muscles to become permanently weakend.